Diabetic Eye Exams
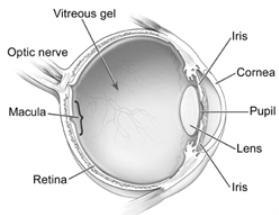
Cross Section of the Eye
Courtesy NIH National Eye Institute
Diabetes can affect the eye and body in a variety of ways. Diabetic eye exams are used to evaluate the effect of diabetes on the retina, on glaucoma, and on the lens of the eye. Below describes the stages of diabetic disease in the eye and how diabetes may affect different systems in the eye.
Lens: One of the earliest effects of diabetes on the eye is with the lens. The lens sits right behind the pupil and is used to focus up close. When blood sugar is high the lens swells and vision may become blurry. This is noticed by the patient as fluctuating vision, typically vision is better in the morning when blood sugar is lower than usual and worse after lunch when blood sugar spikes. This fluctuation generally causes the distance vision to be blurry while the near vision remains ample.
From all this swelling and de-swelling cataracts may form in the lens. This causes a permanent decrease in vision that may be corrected by cataract surgery. See Cataracts
Retina: The retina is the back of the eye and contains photoreceptors for seeing. Blood vessels supply blood to the retina and may be affected by diabetes. During Diabetic Eye Exams the doctor dilate the pupil to get a good view of the retina for leaking blood vessels, areas with a lack of oxygen, swelling of the retina, damage to the optic nerve, fatty deposits, and new blood vessel growth.Diabetic Eye Exams are givenbecause the doctor is able to view the tiny blood vessels in the eye, and changes in the tiny blood vessels of the eye have been shown to represent changes in tiny blood vessels across the body including organs such as the liver and toe. 60-80% of patients with diabetes have at least some diabetic retinopathy after 10 years.
Non-Proliferative Diabetic Retinopathy: NPDR is the first stage of diabetic retinopathy. It is called non-proliferative because there is no new blood vessel growth. NPDR is usually classified as mild, moderate, and severe based on the location and number of bleeds, exudates, cotton wool spots, blood vessel changes, and macular swelling.
In NPDR the thin blood vessels in the retina may become damaged from diabetes and leak. This leakage may result in small bleeds, swelling of the macula which may cause blurred central vision and hard exudates which are fatty deposits in the retina.
Bleeds: These are generally the earliest signs of diabetic retinopathy. The small hemorrhages or bleeds are generally non-vision threatening and may go away in a few days. They start as just a few bleeds and may progress to hundreds. When the bleeds start occurring near the part of the retina called the macula or the central area of the retina, vision may become slightly blurred. These early bleeds are REVERSABLE with better diabetic control.
Clinically Significant Macular Edema: As the blood vessels leak the macula or central part of the retina may become swollen. If this occurs vision may become blurry and distorted. This is distortion is screened by the Amsler Grid. If this occurs laser treatment may be used to seal leaking blood vessels near the central vision.
Another early complication in NPDR is that blood flow may become more sludge like from diabetes and may result in cotton wool spots which are areas of the retina that are not receiving enough oxygen. Cotton wool spots usually occur after the small bleeds. In later stages of NPDR or in proliferative diabetic retinopathy, the cotton wool spots may progress to neovascularization which is new blood vessel growth.
Proliferative Diabetic Retinopathy: PDR has a much greater effect on vision than NPDR. The PDR stage begins when there is neovascularization or new blood vessel growth in the retina. These new vessels occur from lack of oxygen in the retina represented by Cotton Wool Spots in the earlier NPDR stage. The problem with these blood vessels is that they are weak and easily break. This bleeding is much more severe and in a different area of the eye than the bleeding that occurs in NPDR. These new blood vessels may grow into the vitreous or jelly that fills the eye. When the vitreous jelly pulls on these vessels the retina may become detached from the eye or the vessels may break and create large amounts of bleeding. The bleeding may become so severe that the patient may only be able to tell the difference between light and dark in that eye.
Treatment of PDR usually begins with burning holes and killing outer retina and the patient’s peripheral side vision with a laser to decrease oxygen demand to the retina. This decrease in oxygen demand results in fewer weak new blood vessels. If the PDR becomes more severe steroid injections may be used to reduce retinal swelling, anti-VEGF injections may be used to reduce new vessel growth, and removal of the vitreous jelly inside the eye if there is persistent vitreous hemorrhages, retinal detachment, or a large sight threatening bleeds that will not go away.
Neovascular Glaucoma: When diabetes is severely affecting the eye it may result in new blood vessel growth on the iris or front colored part of the eye. These new blood vessels may grow into the drainage system of the eye and result in increased pressure in the eye. This increased pressure may destroy the optic nerve in the back of the eye which sends information to the brain. This process is called glaucoma.
For More Information about Diabetic Eye Exams click Here.
Lens: One of the earliest effects of diabetes on the eye is with the lens. The lens sits right behind the pupil and is used to focus up close. When blood sugar is high the lens swells and vision may become blurry. This is noticed by the patient as fluctuating vision, typically vision is better in the morning when blood sugar is lower than usual and worse after lunch when blood sugar spikes. This fluctuation generally causes the distance vision to be blurry while the near vision remains ample.
From all this swelling and de-swelling cataracts may form in the lens. This causes a permanent decrease in vision that may be corrected by cataract surgery. See Cataracts
Retina: The retina is the back of the eye and contains photoreceptors for seeing. Blood vessels supply blood to the retina and may be affected by diabetes. During Diabetic Eye Exams the doctor dilate the pupil to get a good view of the retina for leaking blood vessels, areas with a lack of oxygen, swelling of the retina, damage to the optic nerve, fatty deposits, and new blood vessel growth.Diabetic Eye Exams are givenbecause the doctor is able to view the tiny blood vessels in the eye, and changes in the tiny blood vessels of the eye have been shown to represent changes in tiny blood vessels across the body including organs such as the liver and toe. 60-80% of patients with diabetes have at least some diabetic retinopathy after 10 years.
Non-Proliferative Diabetic Retinopathy: NPDR is the first stage of diabetic retinopathy. It is called non-proliferative because there is no new blood vessel growth. NPDR is usually classified as mild, moderate, and severe based on the location and number of bleeds, exudates, cotton wool spots, blood vessel changes, and macular swelling.
In NPDR the thin blood vessels in the retina may become damaged from diabetes and leak. This leakage may result in small bleeds, swelling of the macula which may cause blurred central vision and hard exudates which are fatty deposits in the retina.
Bleeds: These are generally the earliest signs of diabetic retinopathy. The small hemorrhages or bleeds are generally non-vision threatening and may go away in a few days. They start as just a few bleeds and may progress to hundreds. When the bleeds start occurring near the part of the retina called the macula or the central area of the retina, vision may become slightly blurred. These early bleeds are REVERSABLE with better diabetic control.
Clinically Significant Macular Edema: As the blood vessels leak the macula or central part of the retina may become swollen. If this occurs vision may become blurry and distorted. This is distortion is screened by the Amsler Grid. If this occurs laser treatment may be used to seal leaking blood vessels near the central vision.
Another early complication in NPDR is that blood flow may become more sludge like from diabetes and may result in cotton wool spots which are areas of the retina that are not receiving enough oxygen. Cotton wool spots usually occur after the small bleeds. In later stages of NPDR or in proliferative diabetic retinopathy, the cotton wool spots may progress to neovascularization which is new blood vessel growth.
Proliferative Diabetic Retinopathy: PDR has a much greater effect on vision than NPDR. The PDR stage begins when there is neovascularization or new blood vessel growth in the retina. These new vessels occur from lack of oxygen in the retina represented by Cotton Wool Spots in the earlier NPDR stage. The problem with these blood vessels is that they are weak and easily break. This bleeding is much more severe and in a different area of the eye than the bleeding that occurs in NPDR. These new blood vessels may grow into the vitreous or jelly that fills the eye. When the vitreous jelly pulls on these vessels the retina may become detached from the eye or the vessels may break and create large amounts of bleeding. The bleeding may become so severe that the patient may only be able to tell the difference between light and dark in that eye.
Treatment of PDR usually begins with burning holes and killing outer retina and the patient’s peripheral side vision with a laser to decrease oxygen demand to the retina. This decrease in oxygen demand results in fewer weak new blood vessels. If the PDR becomes more severe steroid injections may be used to reduce retinal swelling, anti-VEGF injections may be used to reduce new vessel growth, and removal of the vitreous jelly inside the eye if there is persistent vitreous hemorrhages, retinal detachment, or a large sight threatening bleeds that will not go away.
Neovascular Glaucoma: When diabetes is severely affecting the eye it may result in new blood vessel growth on the iris or front colored part of the eye. These new blood vessels may grow into the drainage system of the eye and result in increased pressure in the eye. This increased pressure may destroy the optic nerve in the back of the eye which sends information to the brain. This process is called glaucoma.
For More Information about Diabetic Eye Exams click Here.