Glaucoma
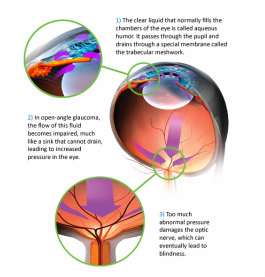
Glaucoma is a disease where the optic nerve dies. The Optic Nerve is the nerve that sends information of what the eyes see to the brain. Why this happens, we are not sure. You may still have 20/20 vision but still have glaucoma! This is because glaucoma is a vision loss disease, not a blur disease. There are many different types of glaucoma; the most common is Primary Open Angle Glaucoma. This goes over the most common types of Glaucoma.
Primary Open Angle Glaucoma: This is the most common type of glaucoma. Most patients start off as Glaucoma Suspects because the disease is diagnosed over multiple visits looking at a number of different data. Glaucoma progresses slowly over years where vision loss starts from the outside and moves in toward the center, it is so slow most patients don’t realize they are going blind. Below are some risk factors you may ask your doctor about.
Family History: Positive family history is a strong risk factor.
Age: Most patients are over the age of 40.
Race: African Americans are most at risk, although it is prevalent across all races.
Pressure: Pressure is believed to have something to do with glaucoma. This is why your pressure is taken at every visit to your eye care professional. We don’t know why but higher and fluctuating pressures tend to correlate with increased nerve damage, this is why the first line of defense is medications that reduce pressure. Pressures between 10 and 20 tend to be normal while pressures above 20 tend to be suspicious, however high pressure does not necessarily mean you have glaucoma and low pressure does not necessarily mean you do not have glaucoma.
Pachymetry: This is used to measure the thickness of the cornea. Greater corneal thickness can give falsely high pressure readings, while thinner corneas can give falsely low pressures meaning patients with thinner corneas are at a higher risk for glaucoma. Corneal thickness of 555 microns is considered average, lower than this is results in increased risk for glaucoma.
Dilation: Dilating the eyes lets us have a good 3-D view of the optic nerve so we can see if there is physical damage and whether or not it is progressing. The doctor looks for tissue damage, bleeding, and the doctor will take measurements of how much nerve tissue vs. space there is at each dilation. This cup to disk ratio or C/D becomes suspicious after about 0.50 and in the case of severe glaucoma can be 0.9 and higher.
Primary Open Angle Glaucoma: This is the most common type of glaucoma. Most patients start off as Glaucoma Suspects because the disease is diagnosed over multiple visits looking at a number of different data. Glaucoma progresses slowly over years where vision loss starts from the outside and moves in toward the center, it is so slow most patients don’t realize they are going blind. Below are some risk factors you may ask your doctor about.
Family History: Positive family history is a strong risk factor.
Age: Most patients are over the age of 40.
Race: African Americans are most at risk, although it is prevalent across all races.
Pressure: Pressure is believed to have something to do with glaucoma. This is why your pressure is taken at every visit to your eye care professional. We don’t know why but higher and fluctuating pressures tend to correlate with increased nerve damage, this is why the first line of defense is medications that reduce pressure. Pressures between 10 and 20 tend to be normal while pressures above 20 tend to be suspicious, however high pressure does not necessarily mean you have glaucoma and low pressure does not necessarily mean you do not have glaucoma.
Pachymetry: This is used to measure the thickness of the cornea. Greater corneal thickness can give falsely high pressure readings, while thinner corneas can give falsely low pressures meaning patients with thinner corneas are at a higher risk for glaucoma. Corneal thickness of 555 microns is considered average, lower than this is results in increased risk for glaucoma.
Dilation: Dilating the eyes lets us have a good 3-D view of the optic nerve so we can see if there is physical damage and whether or not it is progressing. The doctor looks for tissue damage, bleeding, and the doctor will take measurements of how much nerve tissue vs. space there is at each dilation. This cup to disk ratio or C/D becomes suspicious after about 0.50 and in the case of severe glaucoma can be 0.9 and higher.
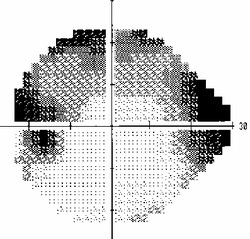
Moderate Glaucomatous Visual Field Defect (loss of vision is shown as darker)
Visual Field: Visual fields let us see how the nerve is functioning. Visual loss starts from the outside and moves in towards the center in a characteristic fashion. Visual fields are repeated to see if there is function of the nerve is deteriorating over time.
OCT/Pictures/Scans: These are used as an objective measure (less subjectivity than seeing the nerve with human eyes) that looks to see if there is nerve damage. These scans are very sensitive and can pick up minor changes year after year.
Gonioscopy: A large contact lens is placed on the eye and through the microscope the drainage pathways for the liquid inside the eye may be seen. If these drainage pathways are narrow there is an increased risk for glaucoma.
Asymmetry: Asymmetric Nerve Head C/D ratios (see Dilation above) or Pressures is cause for suspicion.
Based on all the information above and looking for progression, a doctor may determine whether or not to medicate to slow the optic nerve death. Our only Treatable risk factor is by lowering eye pressure. Treatment begins with eye drops that lower the pressure inside the eye by either draining the liquid in the eye or causing the eye to produce less liquid inside. When glaucoma becomes more severe multiple eye drops affecting different mechanisms to lower pressure are added together. If drops aren’t doing the job well enough different surgeries that open or create alternate drainage passageways to lower the pressure may be done.
OCT/Pictures/Scans: These are used as an objective measure (less subjectivity than seeing the nerve with human eyes) that looks to see if there is nerve damage. These scans are very sensitive and can pick up minor changes year after year.
Gonioscopy: A large contact lens is placed on the eye and through the microscope the drainage pathways for the liquid inside the eye may be seen. If these drainage pathways are narrow there is an increased risk for glaucoma.
Asymmetry: Asymmetric Nerve Head C/D ratios (see Dilation above) or Pressures is cause for suspicion.
Based on all the information above and looking for progression, a doctor may determine whether or not to medicate to slow the optic nerve death. Our only Treatable risk factor is by lowering eye pressure. Treatment begins with eye drops that lower the pressure inside the eye by either draining the liquid in the eye or causing the eye to produce less liquid inside. When glaucoma becomes more severe multiple eye drops affecting different mechanisms to lower pressure are added together. If drops aren’t doing the job well enough different surgeries that open or create alternate drainage passageways to lower the pressure may be done.
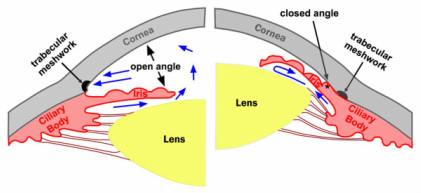
The rt picture shows a closed angle where fluid cannot drain resulting in increased pressure
Angle Closure Glaucoma: Your eye is filled with a jelly and some liquid or Aqueous. Your eye is constantly producing liquid aqueous and draining it through the angle between your Iris (colored part of your eye) and Cornea (clear front part of eye). When this angle is narrow, your eye care professional may refuse to dilate you (this increases the chance of closure) and refer you for surgery. This angle may be looked at by your eye care professional with a Gonio Lens. With age the angle may become narrower because thickening of the lens behind the iris may push the iris forward closer to the cornea, therefore narrowing the angle. Risk Factors include Age, Asian Decent, Female Gender, (+) or Hyperopic Prescriptions, and Family History. To Prevent Angle Closure based on risk factors Laser Peripheral Iridotomy or LPI Surgery is used. This basically is using a laser to put a small hole in the Iris. This allows the aqueous to flow freely without causing a huge increase in pressure. If the angle closes the pressure may shoot up and cause pain, blurred vision, halos, or nausea. Severe nerve damage may occur within a few hours. Treatment is needed immediately and may include breaking the angle closure or giving medication to lower the pressure.
To Learn More about all types of Glaucoma click Here
To Learn More about all types of Glaucoma click Here